


Amid many possibilities of error, it would be strange indeed to be always right. Peter Latham

A complex affair
Providing medical care is a complicated affair. Given the massive number of variables involved (the ability of the patient to provide an accurate history; the expertise of the doctor; the number of health care professionals involved in providing medical care; the difficulty in interpreting test results; and the unpredictable natural history of an illness), it’s hardly surprising that things can go wrong. Anyone who has donned a white coat will tell you what a tough job it is to dedicate your life to the care of anxious patients, especially uneducated ones, or those who do not speak the same language! A good definition of medical error was provided by Dr. James Reason, a Professor of Psychology who describes medical error as – “circumstances in which planned actions fail to achieve the desired outcome”. However, the matter is complicated by the fact that there is no clear-cut definition of what constitutes “gross negligence”, “medical negligence”, “error of judgment”, “accident”, “neglect” or plain “recklessness”!
To err is human
Human error implies that if the medical team member had acted differently, the injury caused to the patient could have been prevented. We all make errors – after all, that’s what makes us human! Jens Rasmussen has suggested that errors occurred due to deficiencies in either one of the following: * Skills (e.g. asking an inexperienced doctor to perform a laparotomy without supervision); * Observation of rules (e.g. not washing hands before performing a procedure); or * Knowledge (e.g. being unaware that gentamicin levels in the blood need to be checked). The truth is that medical errors can occur regardless of a doctor’s vigilance, good intentions, skill, experience or expertise. This is because medical care is a complicated system, and complex systems do fail unpredictably. What we need to do is to work on the system, so that it becomes easier for doctors and other healthcare professionals to go about discharging their duties in a more efficient, error-free manner. The modern approach to patient safety hinges on “systems thinking”- recognition that most errors are made by competent, careful, and caring providers; and that preventing these errors often involves embedding providers in a system that anticipates glitches and catches them before they do harm.
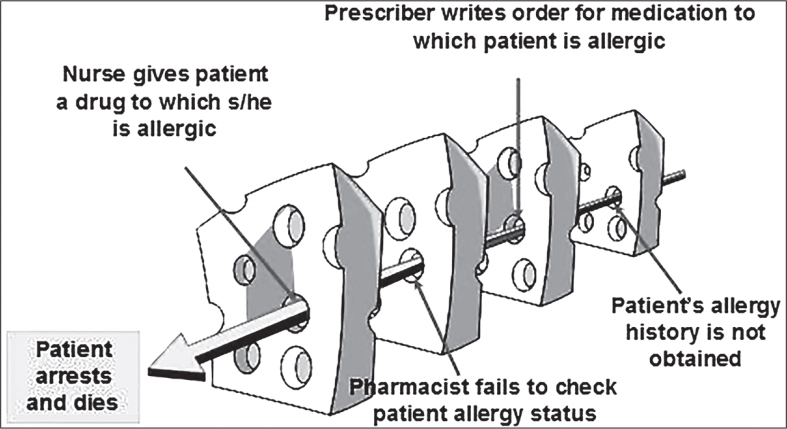
The “Swiss cheese’ model
James Reason, an eminent psychologist, developed the ‘Swiss cheese’ model to explain the multiple factors associated with errors. A wide range of defenses, barriers and safeguards exist to protect patients from hazards. These include basic tools such as alarms on syringe pumps; all the way to sophisticated human error trapping systems, such as anesthetists who check that the surgeon has done a thorough pre-operative work-up of the patient before bringing him to the Operating Room. However, these defenses can be breached, like the holes in slices of Swiss cheese. However, unlike holes in the cheese, these gaps are continually opening, shutting and shifting their location. The presence of holes in any one ‘slice’ does not normally cause a bad outcome. Error happens only when the holes in many layers momentarily line up, bringing hazards into damaging contact with patients. This means that medical error is the result of “system flaws, not character flaws”; and we can reduce human errors by “inserting additional layers of protective cheese into the system”.
Types of errors
This is the dominant model for understanding the relationship between active (“sharp end”) errors and latent (“blunt end”) errors. *
Latent errors
- These are the hidden root causes in the system that make active errors more likely to happen – for example, poorly designed medical records, making it easy for clinicians to misunderstand reports; or inadequate staffing, making people “rush” or routinely “multi- task”. If an individual errs, in a sense she has been set up to fail by her environment. As Don Berwick, President and CEO of the Institute for Healthcare Improvement, has said “every system is perfectly designed to achieve exactly the results it gets.” These defects are difficult to measure because they are hidden, and may exist for years before they are detected.
Active errors
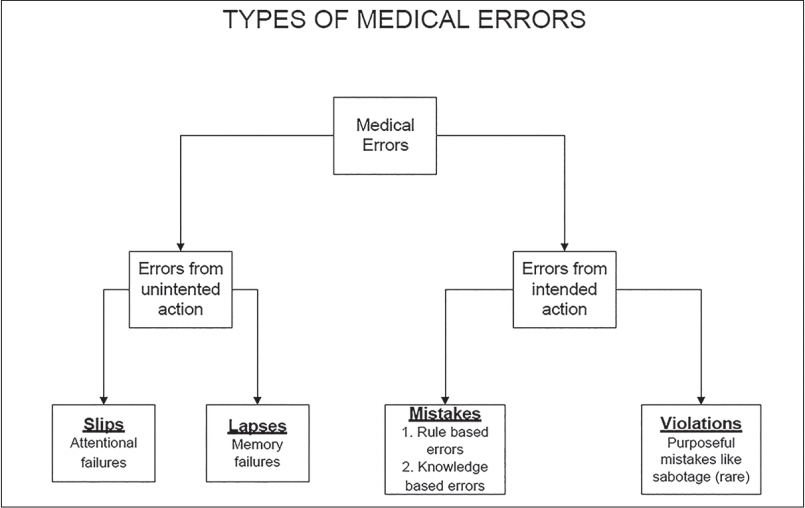
- These occur at the level of the healthcare provider – the frontline staff that actually delivers the services, and can cause harm. These are what we think of when we think of error, due to the focus on individual acts in medicine. Active errors can take the form of slips (doing a familiar action in the wrong way, like pouring salt instead of cream into coffee), lapses (failures of memory such that planned actions do not happen), and mistakes (errors in reasoning that lead to wrong choices). They are easier to measure because the negative outcome is much more apparent – for example, the nurse injects the wrong medication; or the doctor amputates the wrong leg.
A “safety culture” system proactively scans for latent errors all the time, and retroactively looks for latent errors when an active error has occurred. The question should not be – “Who caused the error”, but “What caused the error?” Bad outcomes, just like good outcomes, are a team effort
How can we make the system safer?
Here are some basic principles. * Automate when appropriate * Standardize – reduce reliance on memory * Use checklists & standard operating procedures (SOPs) * Simplify by reducing the number of steps and handoffs * Add redundancy (double checks) for high-risk processes to create a safety net * Stress-test the system, and try to break it, to find out the “failure points” so that these can be reduced and removed * Respect the front-line staff, who are the real-life field experts, and ask them what can be done to help them do their work safely There is a natural tendency for things to go wrong. Safety is a dynamic non-event, and we have to work very hard to ensure nothing bad will happen. Well designed systems can help us to achieve this goal.
Patient Safety from the Patient’s Perspective
The key to patient safety lies in patient empowerment, and there’s a lot that patients can do to protect themselves from medical errors. Patients can use Information Therapy to reduce diagnostic errors; and defend themselves from overtesting and overtreatment. Health literacy is an important safety shield against errors, and patients can use social media to tap into the wisdom of the crowds. Hospitals can be dangerous places, and patients need to use checklists and patient advocates to keep themselves safe when they are hospitalized. And if an error does occur, what steps do you need to take to prevent a bad situation from becoming worse?
I used to be able to find good information from your blog articles.
This is really interesting, You're a very skilled blogger. I've joined your rss feed and look forward to seeking more of your wonderful post. Also, I've shared your website in my social networks!
Hey fantastic website! Does running a blog similar to this take a lot of work? I've virtually no knowledge of programming but I was hoping to start my own blog in the near future. Anyway, should you have any ideas or tips for new blog owners please share. I know this is off subject however I simply wanted to ask. Many thanks!
I'm curious to find out what blog platform you happen to be using? I'm having some minor security problems with my latest blog and I'd like to find something more risk-free. Do you have any solutions?
What's up everyone, it's my first go to see at this website, and post is in fact fruitful in favor of me, keep up posting these articles or reviews.